What’s wrong with how US and Uganda plan to stop Ebola spreading
Published in News & Features



As public health workers in the Democratic Republic of Congo work to rein in a growing outbreak of a rare Ebola virus, other countries are establishing protocols for keeping their own populations safe.
As of May 27, 2026, Congo has reported more than 1,000 suspected and confirmed cases, and more than 250 deaths, according to the U.S. Centers for Disease Control and Prevention. Neighboring Uganda has also reported seven cases and one death. Several Americans who were in the region have been exposed.
Measures such as screening incoming travelers and isolating those who have been exposed, announced by the U.S., Canada and other countries, are scientifically proven ways to effectively address outbreaks.
But recent decisions by two countries stand out because they are not supported by epidemiological evidence – and because they reflect a surprisingly similar way of thinking about outbreak control: On May 27, Uganda closed its border with Congo. Only a narrow set of exceptions apply, mostly for emergency aid workers, and those who cross the border will be subject to health screening and supervised isolation. The following day, the United States announced plans to send exposed Americans from affected countries to a quarantine facility in Kenya, a country with no Ebola cases – though as of May 29, a Kenyan court has blocked the move.
These are very different policies, but both rely on a common assumption: that creating geographic distance from a threat provides protection. However, surveillance, isolation and response capacity are often more important. And both the Ugandan and U.S. moves have drawn criticism from public health and medical experts who argue that managing outbreaks depends more on detection and monitoring than distance alone.
And both decisions emerge from a long-running debate in public health: whether controlling where people are located is more effective than investing in the systems that identify, monitor and treat disease.
As an epidemiologist studying infectious disease outbreaks, I think a look at the history of border restrictions and closures during epidemics helps explain why scientific consensus usually recommends against them.
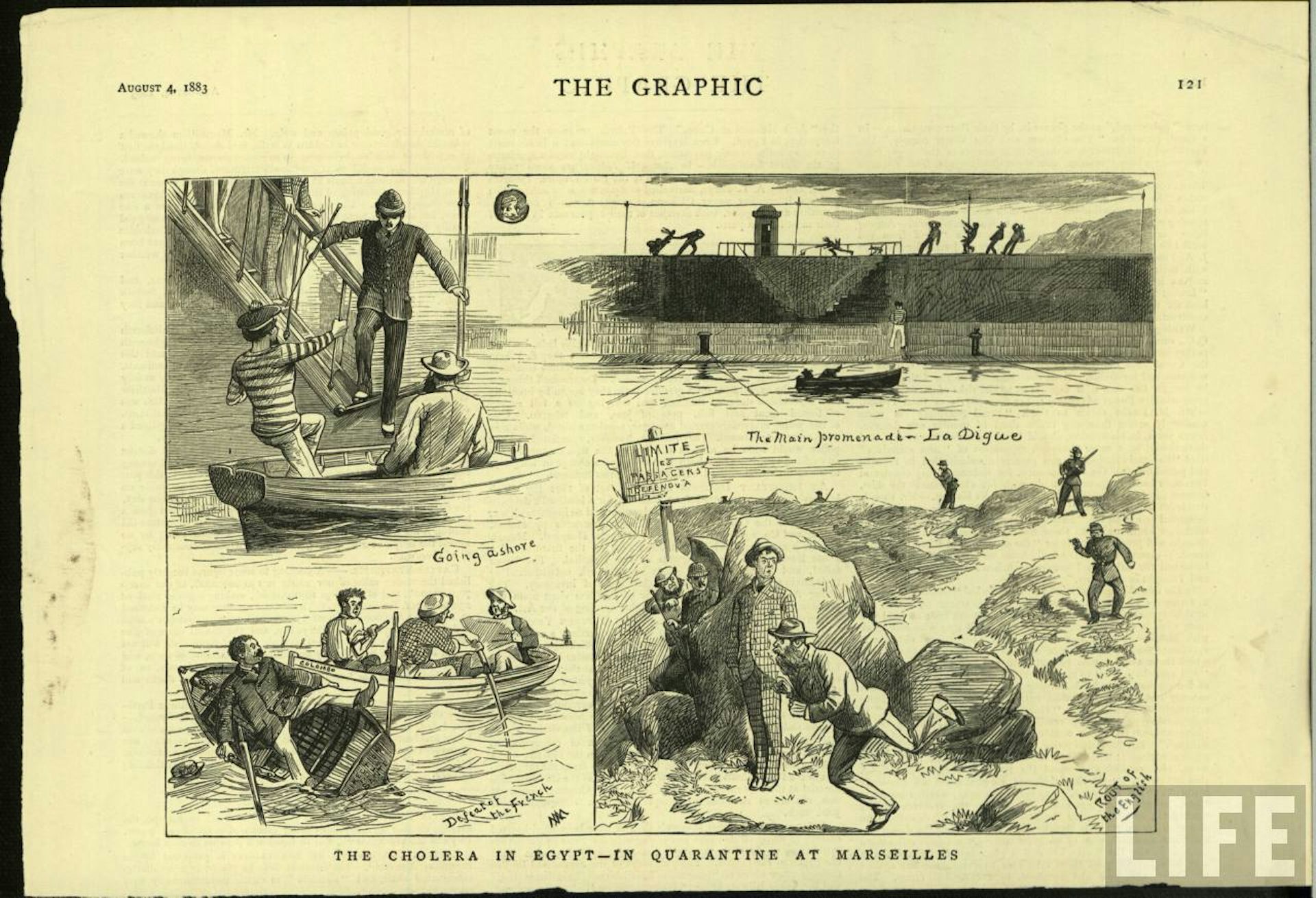
The instinct to seal borders during outbreaks goes back centuries. Venice’s 14th-century “quarantino” was one of the earliest organized attempts by a state to regulate movement in the name of collective health. It worked because the unit of control was a ship: a discrete location that could be anchored offshore for a period of time.
A land border is a fundamentally different problem. As trade networks crossed continents, epidemic control encountered something maritime quarantine never had to solve. You cannot easily anchor people at a land border.
By the 19th century, repeated cholera outbreaks had made the problem international. European powers responded with waves of uncoordinated border closures and trade restrictions that caused enormous economic damage without reliably stopping transmission.
In 1874, governments from around the world met in Vienna for the Fourth International Sanitary Conference to address a problem that sounds remarkably modern: how to control infectious diseases crossing borders without crippling trade and travel. Delegates explicitly rejected border closures and land quarantine as “unworkable and consequently useless.”
The modern descendant of those 19th-century conferences is a set of global laws called the International Health Regulations. Their core purpose is straightforward: Make it safe for countries to report outbreaks honestly, without fear that doing so will trigger economic punishment or travel bans.
The entire modern global health surveillance system rests on a single premise: Countries need to report outbreaks quickly, without fear of automatic economic punishment for doing so. If declaring an outbreak triggers immediate border closures and travel bans, governments have a powerful incentive to delay reporting.
This concern is not hypothetical. During the first SARS outbreak in 2003, China’s delays in official reporting, driven in part by concern about economic fallout, contributed directly to the global spread of the disease. This prompted the World Health Organization to publicly accuse a member state of placing the world at risk. The International Health Regulations were most recently revised in 2005 in direct response to that failure.
When the WHO declared the current Ebola outbreak a public health emergency of international concern on May 17, it explicitly warned against border closures and travel restrictions, saying that these moves “have no basis in science.” That’s because such actions push movement to informal border crossings that are not monitored and “can also compromise local economies and negatively affect response operations from a security and logistics perspective.”
For example, a mother trying to get a sick child to a clinic just across the border may not stop because the formal crossing is shut. The Uganda-Congo border is several hundred miles long and crossed by numerous footpaths beyond formal border posts, which many people use daily to visit family or to trade.
The public health system loses the ability to test, isolate or trace those interactions. This matters especially for Ebola, which transmits only after symptoms begin – meaning a person who can actually spread the virus is already identifiable through symptom screening, making case detection and isolation far more effective than geographic restriction.
The U.S. decision to send exposed Americans to a quarantine facility in Kenya reflects a related instinct – to keep the virus off native soil. But exposure has already occurred, so the public health question is no longer how to prevent entry but how to monitor potentially exposed people safely and effectively. The plan is particularly controversial because it would transfer potentially exposed individuals to a country with no Ebola cases of its own, despite the U.S. already possessing specialized facilities designed for exactly this purpose.
The Infectious Diseases Society of America criticized the plan, noting that the United States has already invested heavily in specialized Ebola treatment centers specifically designed to care for patients with highly dangerous infectious diseases. It warned that building and staffing a new unit in Kenya during an active outbreak raises questions about resources, timing and quality of care.
Some countries did use border closures effectively during COVID-19 – New Zealand, Australia and Taiwan sharply restricted international travel while pairing those measures with intensive testing, quarantine and contact tracing. But specific circumstances made those cases work: restrictions before the virus began spreading widely in the community, island geography that naturally limited informal crossings, and aggressive internal measures running in parallel.
Remove any of those elements and the effectiveness drops sharply. In these examples, the act of closing the border did not work alone. It bought time for setting up the infrastructure for testing and contact tracing.
These circumstances don’t apply to Uganda’s border closing. Researchers estimate the virus had been transmitting for approximately six weeks, and Uganda already has seven confirmed cases. A closure here is not a moat.
Governments face real pressure to act visibly during outbreaks, and border restrictions are easier to communicate to a worried public than investments in surveillance infrastructure. Those incentives are understandable.
But history suggests that outbreaks are controlled less by where people are located than by whether governments can identify cases quickly, trace contacts, isolate infections and maintain public trust. In other words, borders alone do not stop outbreaks. The real work happens inside them.
This article is republished from The Conversation, a nonprofit, independent news organization bringing you facts and trustworthy analysis to help you make sense of our complex world. It was written by: Katrine L. Wallace, University of Illinois Chicago
Read more:
From medieval plague ships to hantavirus: How outbreaks at sea helped to shape the international public health system
I was a nurse on the front lines of Ebola, and I saw that nurses need support for the trauma and pain they experience
Fighting coronavirus fear with empathy: Lessons learned from how Africans got blamed for Ebola
Katrine L. Wallace does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.





Comments